Medical term:
bronchoscopy
Bronchoscopy
Definition
Bronchoscopy is a procedure in which a cylindrical fiberoptic scope is inserted into the airways. This scope contains a viewing device that allows the visual examination of the lower airways.
Purpose
During a bronchoscopy, a physician can visually examine the lower airways, including the larynx, trachea, bronchi, and bronchioles. The procedure is used to examine the mucosal surface of the airways for abnormalities that might be associated with a variety of lung diseases. Its use includes the visualization of airway obstructions such as a tumor, or the collection of specimens for the diagnosis of cancer originating in the bronchi of the lungs (bronchogenic cancer). It can also be used to collect specimens for culture to diagnose infectious diseases such as tuberculosis. The type of specimens collected can include sputum (composed of saliva and discharges from the respiratory passages), tissue samples from the bronchi or bronchioles, or cells collected from washing the lining of the bronchi or bronchioles. The instrument used in bronchoscopy, a bronchoscope, is a slender cylindrical instrument containing a light and an eyepiece. There are two types of bronchoscopes, a rigid tube that is sometimes referred to as an open-tube or ventilating bronchoscope, and a more flexible fiberoptic tube. This tube contains four smaller passages—two for light to pass through, one for seeing through and one that can accommodate medical instruments that may be used for biopsy or suctioning, or that medication can be passed through.
Bronchoscopy may be used for the following purposes:
- to diagnose cancer, tuberculosis, lung infection, or other lung disease
- to examine an inherited deformity of the lungs
- to remove a foreign body in the lungs, such as a mucus plug, tumor, or excessive secretions
- to remove tissue samples, also known as biopsy, to test for cancer cells, help with staging the advancement of the lung cancer, or to treat a tumor with laser therapy
- to allow examination of a suspected tumor, obstruction, secretion, bleeding, or foreign body in the airways
- to determine the cause of a persistent cough, wheezing, or a cough that includes blood in the sputum
- to evaluate the effectiveness of lung cancer treatments
Precautions
Patients not breathing adequately on their own due to severe respiratory failure may require mechanical ventilation prior to bronchoscopy. It may not be appropriate to perform bronchoscopy on patients with an unstable heart condition. All patients must be constantly monitored while undergoing a bronchoscopy so that any abnormal reactions can be dealt with immediately.
Description
There are two types of bronchoscopes, a rigid tube and a fiberoptic tube. Because of its flexibility, the fiberoptic tube is usually preferred. However, if the purpose of the procedure is to remove a foreign body caught in the windpipe or lungs of a child, the more rigid tube must be used because of its larger size. The patient will either lie face-up on his/her back or sit upright in a chair. Medication to decrease secretions, lessen anxiety, and relax the patient are often given prior to the procedure. While breathing through the nose, anesthesia is sprayed into the mouth or nose to numb it. It will take one to two minutes for the anesthesia to take effect. Once this happens, the bronchoscope will be put into the patient's mouth or nose and moved down into the throat. While the bronchoscope is moving down the throat, additional anesthesia is put into the bronchoscope to numb the lower parts of the airways. Using the eyepiece, the physician then observes the trachea and bronchi, and the mucosal lining of these passageways, looking for any abnormalities that may be present.
If the purpose of the bronchoscopy is to take tissue samples or biopsy, forceps or a bronchial brush are used to obtain cells. If the purpose is to identify an infectious agent, a bronchoalveolar lavage (BAL) can be used to gather fluid for culture purposes. Also, if any foreign matter is found in the airways, it can be removed.
Another procedure using bronchoscopy is called fluorescence bronchoscopy. This can be used to detect precancerous cells present in the airways. By using a fluorescent light in the bronchoscope, precancerous tissue will appear dark red, while healthy tissue will appear green. This technique can help detect lung cancer at an early stage, so that treatment can be started early.
Key terms
Anesthesia — A drug used to loss of sensation. It is used to lessen the pain of surgery and medical procedures.
Bronchi — The network of tubular passages that carry air to the lungs and allow air to be expelled from the lungs.
Bronchioles — Small airways extending from the bronchi into the lobes of the lungs.
Bronchoalveolar lavage — Washing cells from the air sacs at the end of the bronchioles.
Trachea — The windpipe.
Alternative procedures
Depending upon the purpose of the bronchoscopy, alternatives might include a computed tomography scan (CT) or no procedure at all. Bronchoscopy is often performed to investigate an abnormality that shows up on a chest x ray or CT scan. If the purpose is to obtain biopsy specimens, one option is to perform surgery, which carries greater risks. Another option is percutaneous (through the skin) biopsy guided by computed tomography.
Preparation
The doctor should be informed of any allergies and all the medications that the patient is currently taking. The doctor may instruct the patient not to take medications like aspirin or anti-inflammatory drugs, which interfere with clotting, for a period of time prior to the procedure. The patient needs to fast for 6 to 12 hours prior to the procedure and refrain from drinking any liquids the day of the procedure. The bronchoscopy takes about 45 to 60 minutes, with results usually available in one day. Prior to the bronchoscopy, several tests may be done, including a chest x ray and blood work. Sometimes a bronchoscopy is done under general anesthesia. Patients usually have an intravenous (IV) line in the arm. Most likely, the procedure will be done under local anesthesia, which is sprayed into the nose or mouth. This is necessary to decrease the gag reflex. A sedative may also be used to help the patient relax. It is important that the patient understands that at no time will the airway be blocked and that oxygen can be supplied through the bronchoscope. A signed consent form is necessary for this procedure.
Aftercare
After the bronchoscopy, the patient will be monitored for vital signs such as heart rate, blood pressure, and breathing, while resting in bed. Sometimes patients have an abnormal reaction to anesthesia. All saliva should be spit into a basin so that it can be examined for the presence of blood. If a biopsy was taken, the patient should not cough or clear the throat as this might dislodge any blood clot that has formed and cause bleeding. No food or drink should be consumed for about two hours after the procedure or until the anesthesia wears off. Diet is gradually progressed from ice chips and clear liquids to the patient's regular diet. There will also be a temporary sore throat and hoarseness that may last for a few days.
Risks
Minor side effects arise from the bronchoscope causing abrasion of the lining of the airways. This results in some swelling and inflammation, as well as hoarseness caused from abrading the vocal cords. If this abrasion is more serious, it can lead to respiratory  difficulty or bleeding of the airway lining. A more serious risk involved in having a bronchoscopy performed is the occurrence of a pneumothorax, due to puncturing of the lungs, which allows air to escape into the space between the lung and the chest wall. These risks are greater with the use of a rigid bronchoscope than with a fiberoptic bronchoscope. If a rigid tube is used, there is also a risk of chipped teeth.
difficulty or bleeding of the airway lining. A more serious risk involved in having a bronchoscopy performed is the occurrence of a pneumothorax, due to puncturing of the lungs, which allows air to escape into the space between the lung and the chest wall. These risks are greater with the use of a rigid bronchoscope than with a fiberoptic bronchoscope. If a rigid tube is used, there is also a risk of chipped teeth.

Bronchoscopy is a procedure in which a hollow, flexible tube is inserted into the airways, allowing the physician to visually examine the lower airways, including the larynx, trachea, bronchi, and bronchioles. It can also be used to collect specimens for bacteriological culture to diagnose infectious diseases such as tuberculosis.
(Illustration by Electronic Illustrators Group.)
Normal results
Normal tracheal appearance consists of smooth muscle with C-shaped rings of cartilage at regular intervals. The trachea and the bronchi are lined with a mucous membrane.
Abnormal results
Abnormal bronchoscopy findings may involve abnormalities of the bronchial wall such as inflammation, swelling, ulceration, or anatomical abnormalities. The bronchoscopy may also reveal the presence of abnormal substances in the trachea and bronchi. If samples are taken, the results could indicate cancer, disease-causing agents or other lung disease. Other abnormalities include constriction or narrowing (stenosis), compression, dilation of vessels, or abnormal branching of the bronchi. Abnormal substances that might be found in the airways include blood, secretions, or mucous plugs. Any abnormalities are discussed with the patient.
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
bronchoscopy
[brong-kos´kah-pe]inspection of the interior of the tracheobronchial tree through a bronchoscope, usually a fiberoptic one passed through the nose. 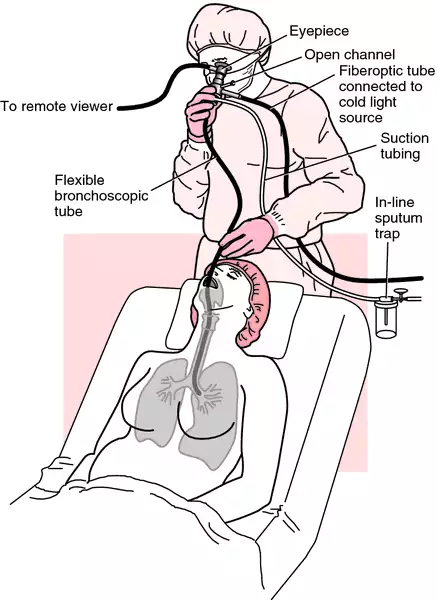 This is used as a diagnostic aid and for therapeutic purposes. As an aid to diagnosis the bronchoscope allows for visualization of the bronchial mucosa and removal of tissue for biopsy. Bronchial washings and collection of secretions are done at the time of bronchoscopy to obtain samples for culture and cytological examination. Therapeutically, the bronchoscope permits removal of foreign bodies that have been aspirated into the bronchial tree and also may be used to facilitate suctioning of the lower airway. The latter technique is done at the bedside and anesthesia is not considered necessary.
This is used as a diagnostic aid and for therapeutic purposes. As an aid to diagnosis the bronchoscope allows for visualization of the bronchial mucosa and removal of tissue for biopsy. Bronchial washings and collection of secretions are done at the time of bronchoscopy to obtain samples for culture and cytological examination. Therapeutically, the bronchoscope permits removal of foreign bodies that have been aspirated into the bronchial tree and also may be used to facilitate suctioning of the lower airway. The latter technique is done at the bedside and anesthesia is not considered necessary.

Flexible fiberoptic bronchoscopy. From Malarkey and McMorrow, 2000.
Patient Care. If the fiberoptic bronchoscope is used at the bedside as an adjunct to bronchial hygiene and removal of secretions, it should be used only by health care personnel who have been trained in the technique. It has the advantage of allowing for more precise suctioning with less trauma to the respiratory tract, because it is possible to visualize the areas needing suctioning and to reach lower segments not accessible to the larger suction catheter.
Bronchoscopy as a surgical diagnostic procedure requires preparation and instruction of patients in regard to the purpose of the procedure, what they can expect to be done, and how they may cooperate during the procedure. A topical anesthetic is used most often, but in some cases the patient may have general anesthesia.
Food and fluids are withheld for 8 hours before bronchoscopy is performed. The teeth should be brushed and the mouth rinsed thoroughly before the procedure to lessen the danger of introducing bacteria from the mouth into the bronchi. Dentures are removed and any loose teeth are brought to the attention of the physician. A mild sedative such as diazepam or midazolam may be given prior to the bronchoscopy. This medication plus instructions to the patient and a full explanation of what is going to be done will help the patient relax and make the passing of the bronchoscope into the bronchi easier and less traumatic.
After bronchoscopy, fluids and food are withheld until the effects of the local anesthetic have worn off and the gag reflex has returned completely. The patient must be observed for signs of bleeding from the throat and respiratory embarrassment. Since swelling of the larynx may necessitate a tracheostomy, the equipment should be readily at hand. The patient should be kept quiet and discouraged from talking or coughing.
Potential problems following bronchoscopy include arterial hypoxemia, bleeding, pneumothorax, bronchial and laryngeal spasm, and anaphylactic reaction to anesthetic drugs.
Bronchospasm and laryngeal spasm necessitate the intravenous administration of medications such as methylprednisolone (Solu-Medrol) and aminophylline. If an intravenous line was not established before the procedure, the equipment should be at the bedside in case it is needed. Indications that bronchospasm is occurring include pallor, respiratory distress, and an elevation of the pulse rate and rate of respirations.
Supplemental oxygen is needed if arterial blood gas analysis or pulse oximetry indicates a drop in the PaO2; hypoxemia can occur either before or after the procedure. Pulse oximetry and electrocardiographic readings are commonly monitored during the procedure. The amount and character of the sputum should be observed in case bleeding occurs, especially when a biopsy has been done during bronchoscopy. A foul-smelling, purulent sputum in the postoperative period probably indicates an infection. A sputum culture for bacteria and an antimicrobial sensitivity test are then commonly ordered.
Pneumothorax is not a common complication of bronchoscopy; should it occur, a thoracotomy tube must be inserted as soon as possible to allow for reexpansion of the lung. A trocar thoracic kit should be readily available.
Bronchoscopy as a surgical diagnostic procedure requires preparation and instruction of patients in regard to the purpose of the procedure, what they can expect to be done, and how they may cooperate during the procedure. A topical anesthetic is used most often, but in some cases the patient may have general anesthesia.
Food and fluids are withheld for 8 hours before bronchoscopy is performed. The teeth should be brushed and the mouth rinsed thoroughly before the procedure to lessen the danger of introducing bacteria from the mouth into the bronchi. Dentures are removed and any loose teeth are brought to the attention of the physician. A mild sedative such as diazepam or midazolam may be given prior to the bronchoscopy. This medication plus instructions to the patient and a full explanation of what is going to be done will help the patient relax and make the passing of the bronchoscope into the bronchi easier and less traumatic.
After bronchoscopy, fluids and food are withheld until the effects of the local anesthetic have worn off and the gag reflex has returned completely. The patient must be observed for signs of bleeding from the throat and respiratory embarrassment. Since swelling of the larynx may necessitate a tracheostomy, the equipment should be readily at hand. The patient should be kept quiet and discouraged from talking or coughing.
Potential problems following bronchoscopy include arterial hypoxemia, bleeding, pneumothorax, bronchial and laryngeal spasm, and anaphylactic reaction to anesthetic drugs.
Bronchospasm and laryngeal spasm necessitate the intravenous administration of medications such as methylprednisolone (Solu-Medrol) and aminophylline. If an intravenous line was not established before the procedure, the equipment should be at the bedside in case it is needed. Indications that bronchospasm is occurring include pallor, respiratory distress, and an elevation of the pulse rate and rate of respirations.
Supplemental oxygen is needed if arterial blood gas analysis or pulse oximetry indicates a drop in the PaO2; hypoxemia can occur either before or after the procedure. Pulse oximetry and electrocardiographic readings are commonly monitored during the procedure. The amount and character of the sputum should be observed in case bleeding occurs, especially when a biopsy has been done during bronchoscopy. A foul-smelling, purulent sputum in the postoperative period probably indicates an infection. A sputum culture for bacteria and an antimicrobial sensitivity test are then commonly ordered.
Pneumothorax is not a common complication of bronchoscopy; should it occur, a thoracotomy tube must be inserted as soon as possible to allow for reexpansion of the lung. A trocar thoracic kit should be readily available.
fiberoptic bronchoscopy bronchofibroscopy.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
bron·chos·co·py
(brong-kos'kŏ-pē),Inspection of the interior of the tracheobronchial tree through a bronchoscope.
Farlex Partner Medical Dictionary © Farlex 2012
bronchoscopy
The use of a flexible endoscope to directly examine the upper airways, vocal cords, and the tracheobronchial tree to the 4th to 6th division.Indications
Evaluate suspected malignancy, haemoptysis, persistent coughing, biopsy (transbronchial) and cytology (e.g., bronchial washings, specimen culture, remove foreign bodies from upper airways).
Relative contraindications
Asthma, severe hypoxia, unstable angina pectoris or recent MI.
Segen's Medical Dictionary. © 2012 Farlex, Inc. All rights reserved.
bronchoscopy
Fiberoptic bronchoscopy The use of a flexible endoscope to directly examine the upper airways, vocal cords, and the tracheobronchial tree to the 4th to 6th division; bronchoscopy is used to evaluate suspected malignancy or infections, hemoptysis, persistent coughing, and occasionally to take biopsies–transbronchial and cytology–eg, bronchial washings, specimen culture and to remove foreign bodies in the upper airways; bronchoscopy should not be performed unless absolutely necessary in Pts with asthma, severe hypoxia, unstable angina pectoris, or recent MI. See Bronchoalveolar lavage, Laser bronchoscopy.Bronchoscopy complications
- Instrument-related
- Common–hemorrhage, pneumothroax, pulmonary infiltrates; rare–air embolism, mediastinal emphysema
- Medication/premedication
- Common–respiratory depression, laryngospasm; rare–bronchospasm, excitability, seizures, hypotension, syncope, cardiorespiratory arrest
- Procedural
- Common–laryngospasm, bronchospasm, hypoxia; uncommon–arrhythmia, fever, bacteremia, pneumonia
- Technical
- Rare–airway, vascular trauma, instrument breakage (Fishman 2nded, 1989, p458)
McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
bron·chos·co·py
(brong-kos'kŏ-pē)Inspection of the interior of the tracheobronchial tree through a bronchoscope.
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
bronchoscopy
Direct visual inspection of the insides of the air tubes (bronchi), either through a hollow metal tube or by means of a fibre optic ENDOSCOPE.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005
bron·chos·co·py
(brong-kos'kŏ-pē)Inspec-tion of the interior of the tracheobronchial tree through a bronchoscope.
Medical Dictionary for the Dental Professions © Farlex 2012
Latest Searches:
zygomaticofrontal - zygomaticofacialis - zygomaticofacial - zygomaticoauricular - zygomatico - zygomatici - zygomatica - zygomatic - zygoma - zygomas - zygodactyly - Zygocotyle - zygion - zygia - zygapophysis - zygapophysiales - zygapophysial - zygapophyseales - zygapophyseal - zygal -
- Service manuals - MBI Corp