Medical term:
midpain
pain
[pān]a feeling of distress, suffering, or agony, caused by stimulation of specialized nerve endings. Its purpose is chiefly protective; it acts as a warning that tissues are being damaged and induces the sufferer to remove or withdraw from the source. The North American Nursing Diagnosis Association has accepted pain as a nursing diagnosis, defining it as a state in which an individual experiences and reports severe discomfort or an uncomfortable sensation; the reporting of pain may be either by direct verbal communication or by encoded descriptors.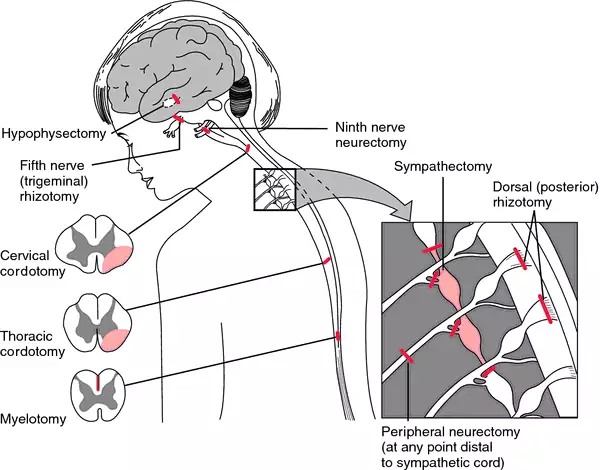
Pain Receptors and Stimuli. All receptors for pain stimuli are free nerve endings of groups of myelinated or unmyelinated neural fibers abundantly distributed in the superficial layers of the skin and in certain deeper tissues such as the periosteum, surfaces of the joints, arterial walls, and the falx and tentorium of the cranial cavity. The distribution of pain receptors in the gastrointestinal mucosa apparently is similar to that in the skin; thus, the mucosa is quite sensitive to irritation and other painful stimuli. Although the parenchyma of the liver and the alveoli of the lungs are almost entirely insensitive to pain, the liver and bile ducts are extremely sensitive, as are the bronchi and parietal pleura.
Some pain receptors are selective in their response to stimuli, but most are sensitive to more than one of the following types of excitation: (1) mechanical stress of trauma; (2) extremes of heat and cold; and (3) chemical substances, such as histamine, potassium ions, acids, prostaglandins, bradykinin, and acetylcholine. Pain receptors, unlike other sensory receptors in the body, do not adapt or become less sensitive to repeated stimulation. Under certain conditions the receptors become more sensitive over a period of time. This accounts for the fact that as long as a traumatic stimulus persists the person will continue to be aware that damage to the tissues is occurring.
The body is able to recognize tissue damage because when cells are destroyed they release the chemical substances previously mentioned. These substances can stimulate pain receptors or cause direct damage to the nerve endings themselves. A lack of oxygen supply to the tissues can also produce pain by causing the release of chemicals from ischemic tissue. Muscle spasm is another cause of pain, probably because it has the indirect effect of causing ischemia and stimulation of chemosensitive pain receptors.
Some pain receptors are selective in their response to stimuli, but most are sensitive to more than one of the following types of excitation: (1) mechanical stress of trauma; (2) extremes of heat and cold; and (3) chemical substances, such as histamine, potassium ions, acids, prostaglandins, bradykinin, and acetylcholine. Pain receptors, unlike other sensory receptors in the body, do not adapt or become less sensitive to repeated stimulation. Under certain conditions the receptors become more sensitive over a period of time. This accounts for the fact that as long as a traumatic stimulus persists the person will continue to be aware that damage to the tissues is occurring.
The body is able to recognize tissue damage because when cells are destroyed they release the chemical substances previously mentioned. These substances can stimulate pain receptors or cause direct damage to the nerve endings themselves. A lack of oxygen supply to the tissues can also produce pain by causing the release of chemicals from ischemic tissue. Muscle spasm is another cause of pain, probably because it has the indirect effect of causing ischemia and stimulation of chemosensitive pain receptors.
Transmission and Recognition of Pain. When superficial pain receptors are excited the impulses are transmitted from these surface receptors to synapses in the gray matter (substantia gelatinosa) of the dorsal horns of the spinal cord. They then travel upward along the sensory pathways to the thalamus, which is the main sensory relay station of the brain. The dorsomedial nucleus of the thalamus projects to the prefrontal cortex of the brain. The conscious perception of pain probably takes place in the thalamus and lower centers; interpretation of the quality of pain is probably the role of the cerebral cortex.
The perception of pain by an individual is highly complex and individualized, and is subject to a variety of external and internal influences. The cerebral cortex is concerned with the appreciation of pain and its quality, location, type, and intensity; thus, an intact sensory cortex is essential to the perception of pain. In addition to neural influences that transmit and modulate sensory input, the perception of pain is affected by psychological and cultural responses to pain-related stimuli. A person can be unaware of pain at the time of an acute injury or other very stressful situation, when in a state of depression, or when experiencing an emotional crisis. Cultural influences also precondition the perception of and response to painful stimuli. The reaction to similar circumstances can range from complete stoicism to histrionic behavior.
The perception of pain by an individual is highly complex and individualized, and is subject to a variety of external and internal influences. The cerebral cortex is concerned with the appreciation of pain and its quality, location, type, and intensity; thus, an intact sensory cortex is essential to the perception of pain. In addition to neural influences that transmit and modulate sensory input, the perception of pain is affected by psychological and cultural responses to pain-related stimuli. A person can be unaware of pain at the time of an acute injury or other very stressful situation, when in a state of depression, or when experiencing an emotional crisis. Cultural influences also precondition the perception of and response to painful stimuli. The reaction to similar circumstances can range from complete stoicism to histrionic behavior.
Pain Control. There are several theories related to the physiologic control of pain but none has been completely verified. One of the best known is that of Mellzak and Wall, the gate control theory, which proposed that pain impulses were mediated in the substantia gelatinosa of the spinal cord with the dorsal horns acting as “gates” that controlled entry of pain signals into the central pain pathways. Also, pain signals would compete with tactile signals with the two constantly balanced against each other.
Since this theory was first proposed, researchers have shown that the neuronal circuitry it hypothesizes is not precisely correct. Nevertheless, there are internal systems that are now known to occur naturally in the body for controlling and mediating pain. One such system, the opioid system, involves the production of morphinelike substances called enkephalins and endorphins. Both are naturally occurring analgesics found in various parts of the brain and spinal cord that are concerned with pain perception and the transmission of pain signals. Signals arising from stimulation of neurons in the gray matter of the brain stem travel downward to the dorsal horns of the spinal cord where incoming pain impulses from the periphery terminate. The descending signals block or significantly reduce the transmission of pain signals upward along the spinal cord to the brain where pain is perceived by releasing these substances.
In addition to the brain's opioid system for controlling the transmission of pain impulses along the spinal cord, there is another mechanism for the control of pain. The stimulation of large sensory fibers extending from the tactile receptors in the skin can suppress the transmission of pain signals from thinner nerve fibers. It is as if the nerve pathways to the brain can accommodate only one type of signal at a time, and when two kinds of impulses simultaneously arrive at the dorsal horns, the tactile sensation takes precedence over the sensation of pain.
The discovery of endorphins and the inhibition of pain transmission by tactile signals has provided a scientific explanation for the effectiveness of such techniques as relaxation, massage, application of liniments, and acupuncture in the control of pain and discomfort.
Since this theory was first proposed, researchers have shown that the neuronal circuitry it hypothesizes is not precisely correct. Nevertheless, there are internal systems that are now known to occur naturally in the body for controlling and mediating pain. One such system, the opioid system, involves the production of morphinelike substances called enkephalins and endorphins. Both are naturally occurring analgesics found in various parts of the brain and spinal cord that are concerned with pain perception and the transmission of pain signals. Signals arising from stimulation of neurons in the gray matter of the brain stem travel downward to the dorsal horns of the spinal cord where incoming pain impulses from the periphery terminate. The descending signals block or significantly reduce the transmission of pain signals upward along the spinal cord to the brain where pain is perceived by releasing these substances.
In addition to the brain's opioid system for controlling the transmission of pain impulses along the spinal cord, there is another mechanism for the control of pain. The stimulation of large sensory fibers extending from the tactile receptors in the skin can suppress the transmission of pain signals from thinner nerve fibers. It is as if the nerve pathways to the brain can accommodate only one type of signal at a time, and when two kinds of impulses simultaneously arrive at the dorsal horns, the tactile sensation takes precedence over the sensation of pain.
The discovery of endorphins and the inhibition of pain transmission by tactile signals has provided a scientific explanation for the effectiveness of such techniques as relaxation, massage, application of liniments, and acupuncture in the control of pain and discomfort.
Assessment of Pain. Pain is a subjective phenomenon that is present when the person who is experiencing it says it is. The person reporting personal discomfort or pain is the most reliable source of information about its location, quality, intensity, onset, precipitating or aggravating factors, and measures that bring relief.
Objective signs of pain can help verify what a patient says about pain, but such data are not used to prove or disprove whether it is present. Physiologic signs of moderate and superficial pain are responses of the sympathetic nervous system. They include rapid, shallow, or guarded respiratory movements, pallor, diaphoresis, increased pulse rate, elevated blood pressure, dilated pupils, and tenseness of the skeletal muscles. Pain that is severe or located deep in body cavities acts as a stimulant to parasympathetic neurons and is evidenced by a drop in blood pressure, slowing of pulse, pallor, nausea and vomiting, weakness, and sometimes a loss of consciousness.
Behavioral signs of pain include crying, moaning, tossing about in bed, pacing the floor, lying quietly but tensely in one position, drawing the knees upward toward the abdomen, rubbing the painful part, and a pinched facial expression or grimacing. The person in pain also may have difficulty concentrating and remembering and may be totally self-centered and preoccupied with the pain.
Psychosocial aspects of tolerance for pain and reactions to it are less easily identifiable and more complex than physiologic responses. An individual's reaction to pain is subject to a variety of psychologic and cultural influences. These include previous experience with pain, training in regard to how one should respond to pain and discomfort, state of health, and the presence of fatigue or physical weakness. One's degree of attention to and distraction from painful stimuli can also affect one's perception of the intensity of pain. A thorough assessment of pain takes into consideration all of these psychosocial factors.
Objective signs of pain can help verify what a patient says about pain, but such data are not used to prove or disprove whether it is present. Physiologic signs of moderate and superficial pain are responses of the sympathetic nervous system. They include rapid, shallow, or guarded respiratory movements, pallor, diaphoresis, increased pulse rate, elevated blood pressure, dilated pupils, and tenseness of the skeletal muscles. Pain that is severe or located deep in body cavities acts as a stimulant to parasympathetic neurons and is evidenced by a drop in blood pressure, slowing of pulse, pallor, nausea and vomiting, weakness, and sometimes a loss of consciousness.
Behavioral signs of pain include crying, moaning, tossing about in bed, pacing the floor, lying quietly but tensely in one position, drawing the knees upward toward the abdomen, rubbing the painful part, and a pinched facial expression or grimacing. The person in pain also may have difficulty concentrating and remembering and may be totally self-centered and preoccupied with the pain.
Psychosocial aspects of tolerance for pain and reactions to it are less easily identifiable and more complex than physiologic responses. An individual's reaction to pain is subject to a variety of psychologic and cultural influences. These include previous experience with pain, training in regard to how one should respond to pain and discomfort, state of health, and the presence of fatigue or physical weakness. One's degree of attention to and distraction from painful stimuli can also affect one's perception of the intensity of pain. A thorough assessment of pain takes into consideration all of these psychosocial factors.
Management of Pain. Among the measures employed to provide relief from pain, administration of analgesic drugs is probably the one that is most often misunderstood and abused. When an analgesic drug has been ordered “as needed,” the patient should know that the drug is truly available when needed and that it will be given promptly when asked for. If the patient is forced to wait until someone else decides when an analgesic is needed, the patient may become angry, resentful, and tense, thus diminishing or completely negating the desired effect of the drug. Studies have shown that when analgesics are left at the bedside of terminally ill cancer patients to be taken at their discretion, fewer doses are taken than when they must rely on someone else to make the drug available. Habituation and addiction to analgesics probably result as much from not using other measures along with analgesics for pain control as from giving prescribed analgesics when they are ordered. Patient-controlled analgesia has been used safely and effectively.
When analgesics are not appropriate or sufficient or when there is a real danger of addiction, there are noninvasive techniques that can be used as alternatives or adjuncts to analgesic therapy. The selection of a particular technique for the management of pain depends on the cause of the pain, its intensity and duration, whether it is acute or chronic, and whether the patient perceives the technique as effective.
Distraction techniques provide a kind of sensory shielding to make the person less aware of discomfort. Distraction can be effective in the relief of brief periods of acute pain, such as that associated with minor surgical procedures under local anesthesia, wound débridement, and venipuncture.
Massage and gentle pressure activate the thick-fiber impulses and produce a preponderance of tactile signals to compete with pain signals. It is interesting that stimulation of the large sensory fibers leading from superficial sensory receptors in the skin can relieve pain at a site distant from the area being rubbed or otherwise stimulated. Since ischemia and muscle spasm can both produce discomfort, massage to improve circulation and frequent repositioning of the body and limbs to avoid circulatory stasis and promote muscle relaxation can be effective in the prevention and management of pain. Transcutaneous electrical nerve stimulation (TENS) units enhance the production of endorphins and enkephalins and can also relieve pain.
Specific relaxation techniques can help relieve physical and mental tension and stress and reduce pain. They have been especially effective in mitigating discomfort during labor and delivery but can be used in a variety of situations. Learning proper relaxation techniques is not easy for some people, but once these techniques have been mastered they can be of great benefit in the management of chronic ongoing pain. The intensity of pain also can be reduced by stimulating the skin through applications of either heat or cold, menthol ointments, and liniments. Contralateral stimulation involves stimulating the skin in an area on the side opposite a painful region. Stimulation can be done by rubbing, massaging, or applying heat or cold.
Since pain is a symptom and therefore of value in diagnosis, it is important to keep accurate records of the observations of the patient having pain. These observations should include the following: the nature of the pain, that is, whether it is described by the patient as being sharp, dull, burning, aching, etc.; the location of the pain, if the patient is able to determine this; the time of onset and the duration, and whether or not certain nursing measures and drugs are successful in obtaining relief; and the relation to other circumstances, such as the position of the patient, occurrence before or after eating, and stimuli in the environment such as heat or cold that may trigger the onset of pain.
When analgesics are not appropriate or sufficient or when there is a real danger of addiction, there are noninvasive techniques that can be used as alternatives or adjuncts to analgesic therapy. The selection of a particular technique for the management of pain depends on the cause of the pain, its intensity and duration, whether it is acute or chronic, and whether the patient perceives the technique as effective.
Distraction techniques provide a kind of sensory shielding to make the person less aware of discomfort. Distraction can be effective in the relief of brief periods of acute pain, such as that associated with minor surgical procedures under local anesthesia, wound débridement, and venipuncture.
Massage and gentle pressure activate the thick-fiber impulses and produce a preponderance of tactile signals to compete with pain signals. It is interesting that stimulation of the large sensory fibers leading from superficial sensory receptors in the skin can relieve pain at a site distant from the area being rubbed or otherwise stimulated. Since ischemia and muscle spasm can both produce discomfort, massage to improve circulation and frequent repositioning of the body and limbs to avoid circulatory stasis and promote muscle relaxation can be effective in the prevention and management of pain. Transcutaneous electrical nerve stimulation (TENS) units enhance the production of endorphins and enkephalins and can also relieve pain.
Specific relaxation techniques can help relieve physical and mental tension and stress and reduce pain. They have been especially effective in mitigating discomfort during labor and delivery but can be used in a variety of situations. Learning proper relaxation techniques is not easy for some people, but once these techniques have been mastered they can be of great benefit in the management of chronic ongoing pain. The intensity of pain also can be reduced by stimulating the skin through applications of either heat or cold, menthol ointments, and liniments. Contralateral stimulation involves stimulating the skin in an area on the side opposite a painful region. Stimulation can be done by rubbing, massaging, or applying heat or cold.
Since pain is a symptom and therefore of value in diagnosis, it is important to keep accurate records of the observations of the patient having pain. These observations should include the following: the nature of the pain, that is, whether it is described by the patient as being sharp, dull, burning, aching, etc.; the location of the pain, if the patient is able to determine this; the time of onset and the duration, and whether or not certain nursing measures and drugs are successful in obtaining relief; and the relation to other circumstances, such as the position of the patient, occurrence before or after eating, and stimuli in the environment such as heat or cold that may trigger the onset of pain.

Surgical procedures designed to alleviate pain. From Ignatavicius et al., 1999.
acute pain
1. one of the three categories of pain established by the International Association for the Study of Pain, denoting pain that is caused by occurrences such as traumatic injury, surgical procedures, or medical disorders; clinical symptoms often include increased heart rate, blood pressure, and respiratory rate, shallow respiration, agitation or restlessness, facial grimaces, or splinting.
2. a nursing diagnosis accepted by the North American Nursing Diagnosis Association, defined as an unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage, with sudden or slow onset of any intensity from mild to severe with an anticipated or predictable end and a duration of less than 6 months.
bearing-down pain pain accompanying uterine contractions during the second stage of labor.
cancer pain one of the three categories of pain established by the International Association for the Study of Pain, denoting pain associated with malignancies and perceived by the individual patient; there are various scales ranking it from 0 to 10 according to level of severity.
chronic pain
1. one of the three categories of pain established by the International Association for the Study of Pain, denoting pain that is persistent, often lasting more than six months; clinical symptoms may be the same as for acute pain, or there may be no symptoms evident. The North American Nursing Diagnosis Association has accepted chronic pain as a nursing diagnosis.
2. a nursing diagnosis accepted by the North American Nursing Diagnosis Association, defined as an unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage, with sudden or slow onset of any intensity from mild to severe, without an anticipated or predictable end, and with a duration of greater than 6 months.
pain disorder a somatoform disorder characterized by a chief complaint of severe chronic pain that causes substantial distress or impairment in functioning; the pain is neither feigned nor intentionally produced, and psychological factors appear to play a major role in its onset, severity, exacerbation, or maintenance. The pain is related to psychological conflicts and is made worse by environmental stress; it enables the patient to avoid an unpleasant activity or to obtain support and sympathy. Patients may visit many health care providers searching for relief and may consume excessive amounts of analgesics without any effect. They are difficult to treat because they strongly resist the idea that their symptoms have a psychological origin.
false p's ineffective pains during pregnancy that resemble labor pains, not accompanied by cervical dilatation; see also braxton-hicks contractions. Called also false labor.
gas p's see gas pains.
growing p's any of various types of recurrent limb pains resembling those of rheumatoid conditions, seen in early youth and formerly thought to be caused by the growing process.
hunger pain pain coming on at the time for feeling hunger for a meal; a symptom of gastric disorder.
intermenstrual pain pain accompanying ovulation, occurring during the period between the menses, usually about midway.
labor p's the rhythmic pains of increasing severity and frequency due to contraction of the uterus at childbirth; see also labor.
lancinating pain sharp darting pain.
phantom pain pain felt as if it were arising in an absent or amputated limb or organ; see also amputation.
psychogenic pain symptoms of physical pain having psychological origin; see pain disorder.
referred pain pain in a part other than that in which the cause that produced it is situated. Referred pain usually originates in one of the visceral organs but is felt in the skin or sometimes in another area deep inside the body. Referred pain probably occurs because pain signals from the viscera travel along the same neural pathways used by pain signals from the skin. The person perceives the pain but interprets it as having originated in the skin rather than in a deep-seated visceral organ.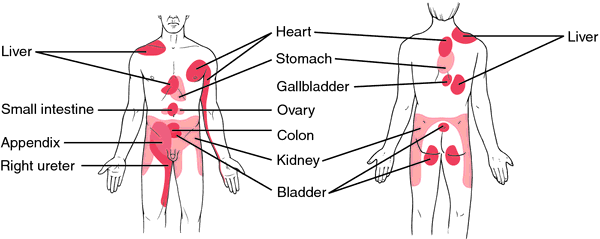

Area of referred pain, anterior and posterior views.
rest pain a continuous unrelenting pain due to ischemia of the lower leg, beginning with or being aggravated by elevation and being relieved by sitting with legs in a dependent position or by standing.
root pain pain caused by disease of the sensory nerve roots and occurring in the cutaneous areas supplied by the affected roots.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
in·ter·men·stru·al pain
1. pelvic discomfort occurring approximately at the time of ovulation, usually at the midpoint of the menstrual cycle; Synonym(s): midpain
2. Synonym(s): mittelschmerz
Farlex Partner Medical Dictionary © Farlex 2012
in·ter·men·stru·al pain
(in'tĕr-men'strū-ăl pān)1. Pelvic discomfort occurring approximately at the time of ovulation, usually at the midpoint of the menstrual cycle.
2. Synonym(s): mittelschmerz.
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
Latest Searches:
zygomaticofrontal - zygomaticofacialis - zygomaticofacial - zygomaticoauricular - zygomatico - zygomatici - zygomatica - zygomatic - zygoma - zygomas - zygodactyly - Zygocotyle - zygion - zygia - zygapophysis - zygapophysiales - zygapophysial - zygapophyseales - zygapophyseal - zygal -
- Service manuals - MBI Corp