Medical term:
radectomy
amputation
[am″pu-ta´shun]the removal of a limb or other appendage or outgrowth of the body. The most common indication for amputation of an upper limb is severe trauma. Blood vessel disorders such as atherosclerosis, often secondary to diabetes mellitus, account for the greatest percentage of amputations of the lower limb. Other indications may include malignancy, infection, and gangrene.
There are two general types of surgical procedure for amputation: (1) the closed or “flap” amputation and (2) the open or “guillotine” amputation. The latter is often required when infection is present and there is a need for free drainage from the operative site. A second surgical procedure involving stump (or residual limb) revision or closure is needed after the guillotine procedure. This is done only after the infection has been eliminated.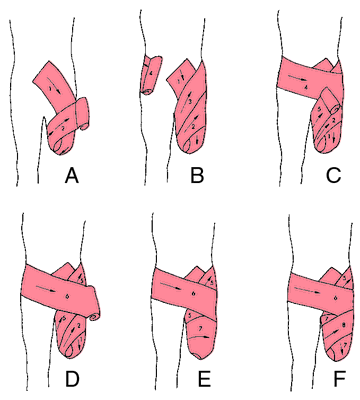
There are two general types of surgical procedure for amputation: (1) the closed or “flap” amputation and (2) the open or “guillotine” amputation. The latter is often required when infection is present and there is a need for free drainage from the operative site. A second surgical procedure involving stump (or residual limb) revision or closure is needed after the guillotine procedure. This is done only after the infection has been eliminated.

Amputation. Bandaging on above-knee amputation stump. A, Use 6" elastic bandage. Enclose medial, distal end of stump. Apply pressure via bandage to end of stump. Use diagonal, not circular turns. B, Turn No. 3 must be high in groin and then turn made around waist to hold No. 3 in place. Do not pull hip into flexion. (A second 6" roll may be needed.) C, Turn No. 5 must be high in groin and a loop made around waist again. D, See diagram. E, Enclose lateral, distal end of stump. (A 4" roll may be needed.) Continue diagonal and figure-of-8 turns around stump. F, Continue turns to shape end of stump. (Courtesy of University of Washington Department of Prosthetics, from booklet Prosthetics-Orthotics.)
Patient Care. The goal of patient care for the amputee is total rehabilitation with attainment of full function and normal active life. Such total rehabilitation is not always possible because of physical and mental limitations of the patient. It requires that the patient be physically and psychologically able to accept and adapt to a prosthesis and that each member of the health care team fulfill his or her responsibilities in preventing complications and in preparing the patient for optimum use of an artificial limb. Some patients, because of age or disease, do not have the necessary energy, muscular coordination, or mental capacity to undertake prosthetic training.
Preoperative Care. Unless time is a factor, as in emergency cases demanding immediate surgery, the preoperative care of the potential amputee should include emotional and vocational aspects as well as the physical. If patients are fully involved in plans for their rehabilitation, understand what is expected of them, and know the regimen of exercise and skills they will need to develop, their chances of full recovery and achievement of independence will be greatly enhanced. Much emotional support and encouragement can be offered by other amputees who are successfully mastering their prosthesis and making progress toward their goal of total rehabilitation.
Patients undergoing amputation will need help in dealing with the changes in body image as they adjust to the loss of a limb. They should be encouraged and given the opportunity to express feelings of anxiety, grief, anger, and depression, and given guidance in working toward a healthy acceptance of their handicap.
In general, physical preparation of the patient undergoing surgical amputation includes measures to promote optimum health and well-being, to establish nutritional and fluid balances, and to increase muscular strength and endurance levels. A program of exercises may be started to help the patient develop skill in using an overhead trapeze, crutches, and a walker and transferring from wheelchair to bed.
Patients undergoing amputation will need help in dealing with the changes in body image as they adjust to the loss of a limb. They should be encouraged and given the opportunity to express feelings of anxiety, grief, anger, and depression, and given guidance in working toward a healthy acceptance of their handicap.
In general, physical preparation of the patient undergoing surgical amputation includes measures to promote optimum health and well-being, to establish nutritional and fluid balances, and to increase muscular strength and endurance levels. A program of exercises may be started to help the patient develop skill in using an overhead trapeze, crutches, and a walker and transferring from wheelchair to bed.
Postoperative Care. The residual limb is watched for hemorrhage, edema, infection, and ischemia. Some bleeding is not unusual but should rarely be more than a modest red stain on the dressing. Ischemia may be caused by a constricting dressing or the development of edema. Ischemia is recognized by the presence of excessive pain.
Traction was formerly commonly used after guillotine amputations but is rarely used nowadays. Generally such stumps are closed by delayed primary closure on the fourth or fifth day after amputation to save time in the hospital and accelerate rehabilitation.
Fitting of a prosthesis may be delayed or immediate depending on the condition of the patient and the reason for the amputation. Immediate fitting of a prosthesis involves the application of a rigid plastic dressing which serves to protect the stump and prevent edema. The dressing is similar to a cast and the patient will require cast care. The temporary prosthetic device is applied at the time of surgery and includes a pylon and foot-ankle assembly.
Early ambulation is a major advantage of immediate fitting of a prosthesis. Other benefits arise from the local compression exerted by the dressing. This serves to inhibit bleeding, to mold and help shrink the stump, and to reduce phantom sensations, pain, and contractures. Unfortunately, not all amputees are candidates for immediate fitting. The technique is not advised for amputations above the knee or above the elbow, for weak and debilitated patients, or for those who are mentally or emotionally unable to cooperate with efforts at rehabilitation. The procedure also requires the services of prosthetic experts.
The more conventional, and probably more frequently chosen, technique of delayed prosthetic fitting requires special care of the stump and a gradual preparation of the patient for weight-bearing and ambulation. During the immediate postoperative period the stump dressings are changed or reinforced as ordered. The stump usually is wrapped with elastic bandages or covered with stump socks. The bandages are checked frequently for signs of bleeding and for slippage, which may lead to a tourniquet effect and the occlusion of blood supply. Exercises are started as soon as possible, regardless of the surgical approach, in order to strengthen the muscles and prevent contractures.
The patient with amputation of an upper limb also may receive immediate or delayed fitting of a prosthesis. When the surgeon has chosen the delayed fitting technique, the patient requires stump care similar to that for the lower limb except that an upper limb stump is bandaged more loosely, especially when amputation was the result of trauma. Exercises are begun the day after surgery and within ten to fourteen days the patient is fitted with a temporary prosthesis.
Traction was formerly commonly used after guillotine amputations but is rarely used nowadays. Generally such stumps are closed by delayed primary closure on the fourth or fifth day after amputation to save time in the hospital and accelerate rehabilitation.
Fitting of a prosthesis may be delayed or immediate depending on the condition of the patient and the reason for the amputation. Immediate fitting of a prosthesis involves the application of a rigid plastic dressing which serves to protect the stump and prevent edema. The dressing is similar to a cast and the patient will require cast care. The temporary prosthetic device is applied at the time of surgery and includes a pylon and foot-ankle assembly.
Early ambulation is a major advantage of immediate fitting of a prosthesis. Other benefits arise from the local compression exerted by the dressing. This serves to inhibit bleeding, to mold and help shrink the stump, and to reduce phantom sensations, pain, and contractures. Unfortunately, not all amputees are candidates for immediate fitting. The technique is not advised for amputations above the knee or above the elbow, for weak and debilitated patients, or for those who are mentally or emotionally unable to cooperate with efforts at rehabilitation. The procedure also requires the services of prosthetic experts.
The more conventional, and probably more frequently chosen, technique of delayed prosthetic fitting requires special care of the stump and a gradual preparation of the patient for weight-bearing and ambulation. During the immediate postoperative period the stump dressings are changed or reinforced as ordered. The stump usually is wrapped with elastic bandages or covered with stump socks. The bandages are checked frequently for signs of bleeding and for slippage, which may lead to a tourniquet effect and the occlusion of blood supply. Exercises are started as soon as possible, regardless of the surgical approach, in order to strengthen the muscles and prevent contractures.
The patient with amputation of an upper limb also may receive immediate or delayed fitting of a prosthesis. When the surgeon has chosen the delayed fitting technique, the patient requires stump care similar to that for the lower limb except that an upper limb stump is bandaged more loosely, especially when amputation was the result of trauma. Exercises are begun the day after surgery and within ten to fourteen days the patient is fitted with a temporary prosthesis.
above-elbow (A-E) amputation amputation of the upper limb between the elbow and the shoulder.
above-knee (A-K) amputation transfemoral amputation.
below-elbow (B-E) amputation amputation of the upper limb between the wrist and the elbow.
below-knee (B-K) amputation transtibial amputation
Chopart's amputation amputation of the foot, with the calcaneus, talus, and other parts of the tarsus being retained.
cineplastic amputation kineplasty.
closed amputation one in which flaps are made from skin and subcutaneous tissue and sutured over the bone end of the stump; called also flap amputation.
congenital amputation absence of a limb at birth, attributed to constriction of the part by an encircling band during intrauterine development.
amputation in contiguity amputation at a joint.
amputation in continuity amputation of a limb elsewhere than at a joint.
Dupuytren's amputation amputation of the upper limb at the shoulder joint.
flap amputation closed amputation.
flapless amputation guillotine amputation.
Gritti-Stokes amputation amputation of the lower limb at the knee through condyles of the femur.
guillotine amputation one in which the entire cross-section is left open (flapless) for dressing; called also flapless or open amputation.
Hey's amputation amputation of the foot between the tarsus and metatarsus.
interpelviabdominal amputation amputation of the lower limb with excision of the lateral portion of the pelvic girdle.
interscapulothoracic amputation amputation of the upper limb with excision of the lateral portion of the shoulder girdle.
kineplastic amputation kineplasty.
Lisfranc's amputation amputation of the foot between the metatarsus and tarsus.
major amputation amputation of the lower limb above the ankle or of the upper limb above the wrist.
minor amputation amputation of a hand or foot, or of a part thereof.
open amputation guillotine amputation.
pulp amputation pulpotomy.
racket amputation one in which there is a single longitudinal incision continuous below with a spiral incision on either side of the limb.
root amputation excision of the root of a tooth; amputation of the root of a single-rooted tooth is called apicoectomy, and that of one root of a two-rooted mandibular tooth is hemisectomy. Called also radectomy and radiectomy.
spontaneous amputation loss of a part without surgical intervention, as in leprosy, ainhum, and certain other conditions.
Syme's amputation disarticulation of the foot with removal of both malleoli.
transfemoral amputation amputation of the lower leg between the knee and the hip. Called also above-knee (A-K) amputation.
transtibial amputation amputation of the lower leg between the ankle and the knee. Called also below-knee (B-K) amputation
traumatic amputation the sudden, accidental removal of a limb or appendage. A limb that is properly cared for may be reimplanted. It should be placed in a plastic bag, and if ice is available the bag containing the limb should be placed in a larger one that contains ice and water.
Tripier's amputation amputation of the foot through the calcaneus.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
root am·pu·ta·tion
surgical removal of one or more roots of a multirooted tooth, the remaining root canal(s) usually being treated endodontically.
Synonym(s): radectomy, radiectomy, radisectomy
Farlex Partner Medical Dictionary © Farlex 2012
radectomy
(rā-dĕk′tə-mē) orradiectomy
(rā′dē-ĕk′tə-mē) orradisectomy
(rā′dĭ-sĕk′tə-mē)n.
See root amputation.
The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
radiectomy
Amputation of a root—e.g., of a nerve or tooth.Segen's Medical Dictionary. © 2012 Farlex, Inc. All rights reserved.
root am·pu·ta·tion
(rūt amp'yū-tā'shŭn)Surgical removal of one or more roots of a multirooted tooth, the remaining root canal(s) usually being treated endodontically.
Synonym(s): radectomy, radiectomy, radicectomy.
Synonym(s): radectomy, radiectomy, radicectomy.
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
root am·pu·ta·tion
(rūt amp'yū-tā'shŭn)Surgical removal of one or more roots of a multirooted tooth; remaining root canal(s) are usually treated endodontically.
Synonym(s): radectomy, radisectomy.
Synonym(s): radectomy, radisectomy.
Medical Dictionary for the Dental Professions © Farlex 2012
Latest Searches:
zymosterol - zymosan - zymoplastic - Zymomonas - zymogenous - zymogenic - zymogen - zymochemistry - Zyme - Zymaxid - Zyloprim - Zymase - Zymar - Zylet - zygotic - zygote - zygotene - zygostyle - zygospore - zygosphere -
- Service manuals - MBI Corp