Medical term:
sanguis
blood
[blud]the fluid that circulates through the heart, arteries, capillaries, and veins and is the chief means of transport within the body. It transports oxygen from the lungs to the body tissues, and carbon dioxide from the tissues to the lungs. It transports nutritive substances and metabolites to the tissues and removes waste products to the kidneys and other organs of excretion. It has an essential role in the maintenance of fluid balance.
In an emergency, blood cells and antibodies carried in the blood are brought to a point of infection, or blood-clotting substances are carried to a break in a blood vessel. The blood distributes hormones from the endocrine glands to the organs they influence. It also helps regulate body temperature by carrying excess heat from the interior of the body to the surface layers of the skin, where the heat is dissipated to the surrounding air.
Blood varies in color from a bright red in the arteries to a duller red in the veins. The total quantity of blood within an individual depends upon body weight; a person weighing 70 kg (154 lb) has about 4.5 liters of blood in the body.
Blood is composed of two parts: the fluid portion is called plasma, and the solid portion or formed elements (suspended in the fluid) consists of the blood cells (erythrocytes and leukocytes) and the platelets. Plasma accounts for about 55 per cent of the volume and the formed elements account for about 45 per cent. ( and table.)
Chemical analyses of various substances in the blood are invaluable aids in (1) the prevention of disease by alerting the patient and health care provider to potentially dangerous levels of blood constituents that could lead to more serious conditions, (2) diagnosis of pathologic conditions already present, (3) assessment of the patient's progress when a disturbance in blood chemistry exists, and (4) assessment of the patient's status by establishing baseline or “normal” levels for each individual patient.
In recent years, with the increasing attention to preventive health care and rapid progress in technology and automation, the use of a battery of screening tests performed by automated instruments has become quite common. These instruments are capable of performing simultaneously a variety of blood chemistry tests. Some of the more common screening tests performed on samples of blood include evaluation of electrolyte, albumin, and bilirubin levels, blood urea nitrogen (BUN), cholesterol, total protein, and such enzymes as lactate dehydrogenase and aspartate transaminase. Other tests include electrophoresis for serum proteins, blood gas analysis, glucose tolerance tests, and measurement of iron levels.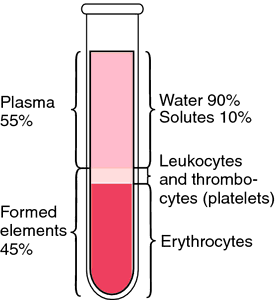
In an emergency, blood cells and antibodies carried in the blood are brought to a point of infection, or blood-clotting substances are carried to a break in a blood vessel. The blood distributes hormones from the endocrine glands to the organs they influence. It also helps regulate body temperature by carrying excess heat from the interior of the body to the surface layers of the skin, where the heat is dissipated to the surrounding air.
Blood varies in color from a bright red in the arteries to a duller red in the veins. The total quantity of blood within an individual depends upon body weight; a person weighing 70 kg (154 lb) has about 4.5 liters of blood in the body.
Blood is composed of two parts: the fluid portion is called plasma, and the solid portion or formed elements (suspended in the fluid) consists of the blood cells (erythrocytes and leukocytes) and the platelets. Plasma accounts for about 55 per cent of the volume and the formed elements account for about 45 per cent. ( and table.)
Chemical analyses of various substances in the blood are invaluable aids in (1) the prevention of disease by alerting the patient and health care provider to potentially dangerous levels of blood constituents that could lead to more serious conditions, (2) diagnosis of pathologic conditions already present, (3) assessment of the patient's progress when a disturbance in blood chemistry exists, and (4) assessment of the patient's status by establishing baseline or “normal” levels for each individual patient.
In recent years, with the increasing attention to preventive health care and rapid progress in technology and automation, the use of a battery of screening tests performed by automated instruments has become quite common. These instruments are capable of performing simultaneously a variety of blood chemistry tests. Some of the more common screening tests performed on samples of blood include evaluation of electrolyte, albumin, and bilirubin levels, blood urea nitrogen (BUN), cholesterol, total protein, and such enzymes as lactate dehydrogenase and aspartate transaminase. Other tests include electrophoresis for serum proteins, blood gas analysis, glucose tolerance tests, and measurement of iron levels.

Composition of the blood, which constitutes 8% of total body weight. From Applegate, 2000.
blood bank
1. a place of storage for blood.
2. an organization that collects, processes, stores, and transfuses blood. In most health agencies the blood bank is located in the pathology laboratory. It is operated by medical technologists under the direction of a pathologist.
blood bank technologist a clinical laboratory scientist/medical technologist who has postgraduate education in blood banking and is certified by the Board of Registry of the American Society of Clinical Pathologists; designated as MT(ASCP)SBB. Specialists in blood bank technology perform both routine and specialized tests in blood bank immunohematology and perform transfusion services. The address of the American Association of Blood Banks is 8101 Glenbrook Road, Bethesda, MD 20814 (telephone 301-907-6582). The address of the Board of Registry of the American Society of Clinical Pathologists is P.O. Box 12270, Chicago, IL 60612. Their telephone number is 312-738-1336 and their web site is http://www.aabb.org.
blood-brain barrier BBB; the barrier separating the blood from the brain parenchyma everywhere except in the hypothalamus. It is permeable to water, oxygen, carbon dioxide, and nonionic solutes, such as glucose, alcohol, and general anesthetics, and is only slightly permeable to electrolytes and other ionic substances. Some small molecules, e.g., amino acids, are taken up across the barrier by specific transport mechanisms.
citrated blood blood treated with sodium citrate or citric acid to prevent its coagulation.
cord blood the blood contained in the umbilical vessels at the time of delivery of the infant. It is rich in stem cells that could be used in place of bone marrow for a transplant; thus, it is sometimes collected and stored for future use.
blood count determination of the number of blood cells in a given sample of blood, usually expressed as the number in a cubic millimeter; it may be either a complete blood count or a count of just one of the elements such as an erythrocyte count, leukocyte count or a platelet count. Methods include manual counts using a hemacytometer and automated counts using a flow cytometer, a Coulter counter, or other means. The blood count is useful in the diagnosis of various blood dyscrasias, infections, or other abnormal conditions and is one of the most common tests done on the blood. Called also blood cell count. (See accompanying table.)
defibrinated blood whole blood from which fibrin has been separated during the clotting process.
blood gas analysis laboratory studies of arterial and venous blood for the purpose of measuring oxygen and carbon dioxide levels and pressure or tension, and hydrogen ion concentration (pH). (See accompanying table.) Analyses of blood gases provide the following information:ƒ
PaO2—partial pressure (P) of oxygen (O2) in the arterial blood (a)
SaO2—percentage of available hemoglobin that is saturated (Sa) with oxygen (O2)
PaCO2—partial pressure (P) of carbon dioxide (CO2) in the arterial blood (a)
pH—an expression of the extent to which the blood is alkaline or acidic
HCO3−—the level of plasma bicarbonate; an indicator of the metabolic acid-base status
These parameters are important tools for assessment of a patient's acid-base balance. They reflect the ability of the lungs to exchange oxygen and carbon dioxide, the ability of the kidneys to control the retention or elimination of bicarbonate, and the effectiveness of the heart as a pump. Because the lungs and kidneys act as important regulators of the respiratory and metabolic acid-base balance, assessment of the status of a patient with any disorder of respiration and metabolism includes periodic blood gas measurements.
The partial pressure of a particular gas in a mixture of gases, as of oxygen in air, is the pressure exerted by that gas alone. It is proportional to the relative number of molecules of the gas, for example, the fraction of all the molecules in the air that are oxygen molecules. The partial pressure of a gas in a liquid is the partial pressure of a real or imaginary gas that is in equilibrium with the liquid.
PaO2 measures the oxygen content of the arterial blood, most of which is bound to hemoglobin, forming oxyhemoglobin. The SaO2 measures the oxygen in oxyhemoglobin as a percentage of the total hemoglobin oxygen-carrying capacity.
A PaO2 of 60 mm Hg represents an SaO2 of 90 per cent, which is sufficient to meet the needs of the body's cells. However, as the PaO2 falls, the SaO2 decreases rapidly. A PaO2 below 55 indicates a state of hypoxemia that requires correction. Normal PaO2 values at sea level are 80 mm Hg for elderly adults and 100 mm Hg for young adults.
However, some patients with chronic obstructive pulmonary disease can tolerate a PaO2 as low as 70 mm Hg without becoming hypoxic. In caring for patients with this condition, it is important to know that attempts to elevate the PaO2 level to the normal level can be dangerous and even fatal. It is best to establish a baseline for each individual patient before supplementary oxygen is given, and then to assess his condition and the effectiveness of his therapy according to this baseline.
The PaCO2 gives information about the cellular production of carbon dioxide through metabolic processes, and the removal of it from the body via the lungs. The normal range is 32 to 45 mm Hg. Values outside this range indicate a primary respiratory problem associated with pulmonary function, or a metabolic problem for which there is respiratory compensation.
In the newborn the normal PaO2 is 50 to 80 mm Hg. At 40 to 50 mm Hg cyanosis may become apparent. Respiratory distress in an infant who is unable to ventilate the lungs adequately will produce a drop in PaO2 level. However, there is no marked increase in PaCO2 level in some infants as in adults with respiratory distress because many infants can still eliminate carbon dioxide from the lungs even though weakness prevents inhaling an adequate oxygen supply. All infants being ventilated and receiving oxygen therapy require frequent blood gas analyses and also pH, base excess, and oxygen saturation levels to avoid oxygen toxicity and acid-base imbalance.
Blood pH gives information about the patient's metabolic state. A pH of 7.4 is considered normal; a value lower than 7.4 indicates acidemia and one higher than 7.4 alkalemia.
Because the amount of CO2 in the blood affects its pH, abnormal PaCO2 values are interpreted in relation to the pH. If the PaCO2 value is elevated, and the pH is below normal, respiratory acidosis from either acute or chronic hyperventilation is suspected. Conversely, a PaCO2 below normal and a pH above normal indicates respiratory alkalosis. When both the PaCO2 and the pH are elevated, there is respiratory retention of CO2 to compensate for metabolic acidosis. If both values are below normal, there is respiratory elimination of CO2 (hyperventilation) to compensate for metabolic acidosis.
Abnormal levels of bicarbonate (HCO3−) in the plasma are also interpreted in relation to the pH in the diagnosis of disturbances in the metabolic component of the acid-base balance. The normal range for HCO3− is 22 to 26 mEq per liter. Abnormally low levels of both HCO3− and pH indicate acidosis of metabolic origin. Conversely, elevations of both of these values indicate metabolic alkalosis. The kidneys maintain bicarbonate levels by filtering bicarbonate and returning it to the blood; they also produce new bicarbonate to replace that which is used in buffering. Therefore, a decreased HCO3− and an increased pH level indicate either retention of hydrogen ions by the kidneys or the elimination of HCO3− in an effort to compensate for respiratory alkalosis. Conversely, if the HCO3− level is increased and the pH is decreased, the kidneys have compensated for respiratory acidosis by retaining HCO3− or by eliminating hydrogen ions.
PaO2—partial pressure (P) of oxygen (O2) in the arterial blood (a)
SaO2—percentage of available hemoglobin that is saturated (Sa) with oxygen (O2)
PaCO2—partial pressure (P) of carbon dioxide (CO2) in the arterial blood (a)
pH—an expression of the extent to which the blood is alkaline or acidic
HCO3−—the level of plasma bicarbonate; an indicator of the metabolic acid-base status
These parameters are important tools for assessment of a patient's acid-base balance. They reflect the ability of the lungs to exchange oxygen and carbon dioxide, the ability of the kidneys to control the retention or elimination of bicarbonate, and the effectiveness of the heart as a pump. Because the lungs and kidneys act as important regulators of the respiratory and metabolic acid-base balance, assessment of the status of a patient with any disorder of respiration and metabolism includes periodic blood gas measurements.
The partial pressure of a particular gas in a mixture of gases, as of oxygen in air, is the pressure exerted by that gas alone. It is proportional to the relative number of molecules of the gas, for example, the fraction of all the molecules in the air that are oxygen molecules. The partial pressure of a gas in a liquid is the partial pressure of a real or imaginary gas that is in equilibrium with the liquid.
PaO2 measures the oxygen content of the arterial blood, most of which is bound to hemoglobin, forming oxyhemoglobin. The SaO2 measures the oxygen in oxyhemoglobin as a percentage of the total hemoglobin oxygen-carrying capacity.
A PaO2 of 60 mm Hg represents an SaO2 of 90 per cent, which is sufficient to meet the needs of the body's cells. However, as the PaO2 falls, the SaO2 decreases rapidly. A PaO2 below 55 indicates a state of hypoxemia that requires correction. Normal PaO2 values at sea level are 80 mm Hg for elderly adults and 100 mm Hg for young adults.
However, some patients with chronic obstructive pulmonary disease can tolerate a PaO2 as low as 70 mm Hg without becoming hypoxic. In caring for patients with this condition, it is important to know that attempts to elevate the PaO2 level to the normal level can be dangerous and even fatal. It is best to establish a baseline for each individual patient before supplementary oxygen is given, and then to assess his condition and the effectiveness of his therapy according to this baseline.
The PaCO2 gives information about the cellular production of carbon dioxide through metabolic processes, and the removal of it from the body via the lungs. The normal range is 32 to 45 mm Hg. Values outside this range indicate a primary respiratory problem associated with pulmonary function, or a metabolic problem for which there is respiratory compensation.
In the newborn the normal PaO2 is 50 to 80 mm Hg. At 40 to 50 mm Hg cyanosis may become apparent. Respiratory distress in an infant who is unable to ventilate the lungs adequately will produce a drop in PaO2 level. However, there is no marked increase in PaCO2 level in some infants as in adults with respiratory distress because many infants can still eliminate carbon dioxide from the lungs even though weakness prevents inhaling an adequate oxygen supply. All infants being ventilated and receiving oxygen therapy require frequent blood gas analyses and also pH, base excess, and oxygen saturation levels to avoid oxygen toxicity and acid-base imbalance.
Blood pH gives information about the patient's metabolic state. A pH of 7.4 is considered normal; a value lower than 7.4 indicates acidemia and one higher than 7.4 alkalemia.
Because the amount of CO2 in the blood affects its pH, abnormal PaCO2 values are interpreted in relation to the pH. If the PaCO2 value is elevated, and the pH is below normal, respiratory acidosis from either acute or chronic hyperventilation is suspected. Conversely, a PaCO2 below normal and a pH above normal indicates respiratory alkalosis. When both the PaCO2 and the pH are elevated, there is respiratory retention of CO2 to compensate for metabolic acidosis. If both values are below normal, there is respiratory elimination of CO2 (hyperventilation) to compensate for metabolic acidosis.
Abnormal levels of bicarbonate (HCO3−) in the plasma are also interpreted in relation to the pH in the diagnosis of disturbances in the metabolic component of the acid-base balance. The normal range for HCO3− is 22 to 26 mEq per liter. Abnormally low levels of both HCO3− and pH indicate acidosis of metabolic origin. Conversely, elevations of both of these values indicate metabolic alkalosis. The kidneys maintain bicarbonate levels by filtering bicarbonate and returning it to the blood; they also produce new bicarbonate to replace that which is used in buffering. Therefore, a decreased HCO3− and an increased pH level indicate either retention of hydrogen ions by the kidneys or the elimination of HCO3− in an effort to compensate for respiratory alkalosis. Conversely, if the HCO3− level is increased and the pH is decreased, the kidneys have compensated for respiratory acidosis by retaining HCO3− or by eliminating hydrogen ions.
blood gas analysis, mixed venous blood gas analysis performed on a blood sample obtained from the pulmonary artery.
blood gas analysis, transcutaneous the determination of PO2 and PCO2 by placement of a heated electrode over the skin to get an inference of PaO2 and PaCO2.
blood group the phenotype of erythrocytes defined by one or more cellular antigenic structural groupings under the control of allelic genes. In clinical practice there are four main blood groups or blood types: A, B, O, and AB (see table). In addition to this major grouping there is an Rh-hR system that is important in the prevention of erythroblastosis fetalis resulting from incompatibility of blood groups in mother and fetus.
The ABO blood group system was first introduced in 1900 by Karl Landsteiner; in 1920 group AB was discovered by van Descatello and Sturli. Identification of these four major blood groups represented a major step toward resolving the problem of blood transfusion reactions resulting from donor-recipient incompatibility. In 1938 Landsteiner and Weiner discovered another blood factor related to maternal-fetal incompatibility. The factor was named Rh because the researchers were using rhesus monkeys in their studies. Further research has uncovered additional factors in the Rh group.
Although more than 90 factors have been identified, many of these are not highly antigenic and are not, therefore, a cause for concern in the typing of blood for clinical purposes.
The term factor, in reference to blood groups, is synonymous with antigen, and the reaction occurring between incompatible blood types is an antigen-antibody reaction. In cases of incompatibility, the antigen, located on the red blood cells, is an agglutinogen and the specific antibody, located in the serum, is an agglutinin. These are so named because whenever red blood cells with a certain factor come in contact with the agglutinin specific for it, there is agglutination or clumping of the erythrocytes.
In determining blood group, a sample of blood is taken and mixed with specially prepared sera. One serum, anti-A agglutinin, causes blood of group A to agglutinate; another serum, anti-B agglutinin, causes blood of group B to agglutinate. Thus, if anti-A serum alone causes clumping, the blood is group A; if anti-B serum alone causes clumping, it is group B. If both cause clumping, the blood group is AB, and if it is not clumped by either, it is identified as group O.
The ABO blood group system was first introduced in 1900 by Karl Landsteiner; in 1920 group AB was discovered by van Descatello and Sturli. Identification of these four major blood groups represented a major step toward resolving the problem of blood transfusion reactions resulting from donor-recipient incompatibility. In 1938 Landsteiner and Weiner discovered another blood factor related to maternal-fetal incompatibility. The factor was named Rh because the researchers were using rhesus monkeys in their studies. Further research has uncovered additional factors in the Rh group.
Although more than 90 factors have been identified, many of these are not highly antigenic and are not, therefore, a cause for concern in the typing of blood for clinical purposes.
The term factor, in reference to blood groups, is synonymous with antigen, and the reaction occurring between incompatible blood types is an antigen-antibody reaction. In cases of incompatibility, the antigen, located on the red blood cells, is an agglutinogen and the specific antibody, located in the serum, is an agglutinin. These are so named because whenever red blood cells with a certain factor come in contact with the agglutinin specific for it, there is agglutination or clumping of the erythrocytes.
In determining blood group, a sample of blood is taken and mixed with specially prepared sera. One serum, anti-A agglutinin, causes blood of group A to agglutinate; another serum, anti-B agglutinin, causes blood of group B to agglutinate. Thus, if anti-A serum alone causes clumping, the blood is group A; if anti-B serum alone causes clumping, it is group B. If both cause clumping, the blood group is AB, and if it is not clumped by either, it is identified as group O.
occult blood that present in such small amounts as to be detectable only by chemical tests or by spectroscopic or microscopic examination.
peripheral blood that obtained from acral areas, or from the circulation remote from the heart; the blood in the systemic circulation.
blood poisoning popular term for septicemia.
blood pressure
1. the pressure of the blood against the walls of any blood vessel.
2. the term usually refers to the pressure of the blood within the arteries, or arterial blood pressure. This pressure is determined by several interrelated factors, including the pumping action of the heart, the resistance to the flow of blood in the arterioles, the elasticity of the walls of the main arteries, the blood volume and extracellular fluid volume, and the blood's viscosity, or thickness.
The pumping action of the heart refers to how hard the heart pumps the blood (force of heartbeat), how much blood it pumps (the cardiac output), and how efficiently it does the job. Contraction of the heart, which forces blood through the arteries, is the phase known as systole. Relaxation of the heart between contractions is called diastole.
The main arteries leading from the heart have walls with strong elastic fibers capable of expanding and absorbing the pulsations generated by the heart. At each pulsation the arteries expand and absorb the momentary increase in blood pressure. As the heart relaxes in preparation for another beat, the aortic valves close to prevent blood from flowing back to the heart chambers, and the artery walls spring back, forcing the blood through the body between contractions. In this way the arteries act as dampers on the pulsations and thus provide a steady flow of blood through the blood vessels. Because of this, there are actually two blood pressures within the blood vessels during one complete beat of the heart: a higher blood pressure during systole (the contraction phase) and a lower blood pressure during diastole (the relaxation phase). These two blood pressures are known as the systolic pressure and the diastolic pressure, respectively.
It is generally agreed that a reading of 120 mm Hg systolic and 80 mm Hg diastolic are the norms for a blood pressure reading; that is, it represents the average blood pressure obtained from a large sampling of healthy adults. In general, a blood pressure of 95 mm Hg systolic and 60 mm Hg diastolic indicates hypotension. However, a reading equal to or below this level must be interpreted in the light of each patient's “normal” reading as determined by baseline data.
On the basis of validated research on the long-term effects of an elevated blood pressure, it is generally agreed that some degree of risk for major cardiovascular disease exists when the systolic pressure is greater than or equal to 140 mm Hg, and the diastolic pressure is greater than or equal to 90 mm Hg. Life expectancy is reduced at all ages and in both males and females when the diastolic pressure is above 90 mm Hg. (See accompanying table.)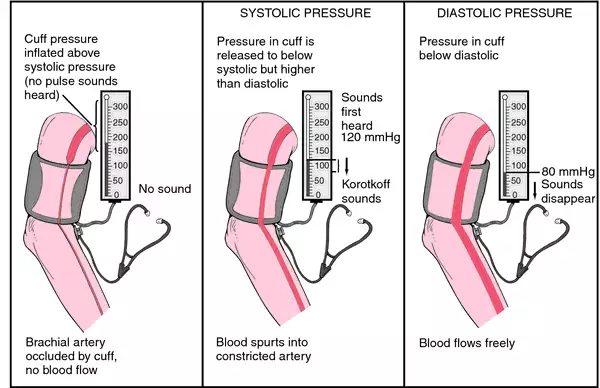 This consists of a rubber cuff and a gauge or column of mercury for measuring pressure. The rubber cuff is wrapped about the patient's arm, and then air is pumped into the cuff by means of a rubber bulb. As the pressure inside the rubber cuff increases, the flow of blood through the artery is momentarily checked.
This consists of a rubber cuff and a gauge or column of mercury for measuring pressure. The rubber cuff is wrapped about the patient's arm, and then air is pumped into the cuff by means of a rubber bulb. As the pressure inside the rubber cuff increases, the flow of blood through the artery is momentarily checked.
A stethoscope is placed over the artery at the elbow and the air pressure within the cuff is slowly released. As soon as blood begins to flow through the artery again, Korotkoff sounds are heard. The first sounds heard are tapping sounds that gradually increase in intensity. The initial tapping sound that is heard for at least two consecutive beats is recorded as the systolic blood pressure.
The first phase of the sounds may be followed by a momentary disappearance of sounds that can last from 30 to 40 mm Hg as the gauge needle (or mercury column) descends. It is important that this auscultatory gap not be missed; otherwise, either an erroneously low systolic pressure or high diastolic pressure will be obtained.
During the second phase following the temporary absence of sound there are murmuring or swishing sounds. As deflation of the cuff continues, the sounds become sharper and louder. These sounds represent phase three. During phase four the sounds become muffled rather abruptly and then are followed by silence, which represents phase five.
Although there is disagreement as to which of the latter phases should represent the diastolic pressure, it is usually recommended that phase five, the point at which sounds disappear, be used as the diastolic pressure for adults, and phase four be used for children. The reason for this is that children, having a high cardiac output, often will continue to produce sounds when the gauge is at a very low reading or even at zero. In some adult patients whose arterioles have lost their elasticity, the fifth phase is also extremely low or nonexistent. In these cases, it is recommended that three readings be recorded: phase one and phases four and five. For example, the blood pressure would be written as 140/96/0. On most occasions, however, the blood pressure is written as a fraction. The systolic pressure is written as the top number, a line is drawn, and the diastolic pressure is written as the bottom number.
Errors in blood pressure measurement can result from failure of the cuff to reach and compress the artery. The cuff diameter should be 20 per cent greater than the diameter of the limb, the bladder of the cuff must be centered over the artery, and the cuff must be wrapped smoothly and snugly to ensure proper inflation. When a mercury gauge is used, the meniscus should be at eye level to avoid a false reading.
The pumping action of the heart refers to how hard the heart pumps the blood (force of heartbeat), how much blood it pumps (the cardiac output), and how efficiently it does the job. Contraction of the heart, which forces blood through the arteries, is the phase known as systole. Relaxation of the heart between contractions is called diastole.
The main arteries leading from the heart have walls with strong elastic fibers capable of expanding and absorbing the pulsations generated by the heart. At each pulsation the arteries expand and absorb the momentary increase in blood pressure. As the heart relaxes in preparation for another beat, the aortic valves close to prevent blood from flowing back to the heart chambers, and the artery walls spring back, forcing the blood through the body between contractions. In this way the arteries act as dampers on the pulsations and thus provide a steady flow of blood through the blood vessels. Because of this, there are actually two blood pressures within the blood vessels during one complete beat of the heart: a higher blood pressure during systole (the contraction phase) and a lower blood pressure during diastole (the relaxation phase). These two blood pressures are known as the systolic pressure and the diastolic pressure, respectively.
It is generally agreed that a reading of 120 mm Hg systolic and 80 mm Hg diastolic are the norms for a blood pressure reading; that is, it represents the average blood pressure obtained from a large sampling of healthy adults. In general, a blood pressure of 95 mm Hg systolic and 60 mm Hg diastolic indicates hypotension. However, a reading equal to or below this level must be interpreted in the light of each patient's “normal” reading as determined by baseline data.
On the basis of validated research on the long-term effects of an elevated blood pressure, it is generally agreed that some degree of risk for major cardiovascular disease exists when the systolic pressure is greater than or equal to 140 mm Hg, and the diastolic pressure is greater than or equal to 90 mm Hg. Life expectancy is reduced at all ages and in both males and females when the diastolic pressure is above 90 mm Hg. (See accompanying table.)
Measurement of the Blood Pressure. The blood pressure is usually measured in the artery of the upper arm, with a sphygmomanometer.

Measurement of blood pressure. From Applegate, 2000.
A stethoscope is placed over the artery at the elbow and the air pressure within the cuff is slowly released. As soon as blood begins to flow through the artery again, Korotkoff sounds are heard. The first sounds heard are tapping sounds that gradually increase in intensity. The initial tapping sound that is heard for at least two consecutive beats is recorded as the systolic blood pressure.
The first phase of the sounds may be followed by a momentary disappearance of sounds that can last from 30 to 40 mm Hg as the gauge needle (or mercury column) descends. It is important that this auscultatory gap not be missed; otherwise, either an erroneously low systolic pressure or high diastolic pressure will be obtained.
During the second phase following the temporary absence of sound there are murmuring or swishing sounds. As deflation of the cuff continues, the sounds become sharper and louder. These sounds represent phase three. During phase four the sounds become muffled rather abruptly and then are followed by silence, which represents phase five.
Although there is disagreement as to which of the latter phases should represent the diastolic pressure, it is usually recommended that phase five, the point at which sounds disappear, be used as the diastolic pressure for adults, and phase four be used for children. The reason for this is that children, having a high cardiac output, often will continue to produce sounds when the gauge is at a very low reading or even at zero. In some adult patients whose arterioles have lost their elasticity, the fifth phase is also extremely low or nonexistent. In these cases, it is recommended that three readings be recorded: phase one and phases four and five. For example, the blood pressure would be written as 140/96/0. On most occasions, however, the blood pressure is written as a fraction. The systolic pressure is written as the top number, a line is drawn, and the diastolic pressure is written as the bottom number.
Errors in blood pressure measurement can result from failure of the cuff to reach and compress the artery. The cuff diameter should be 20 per cent greater than the diameter of the limb, the bladder of the cuff must be centered over the artery, and the cuff must be wrapped smoothly and snugly to ensure proper inflation. When a mercury gauge is used, the meniscus should be at eye level to avoid a false reading.
Direct Measurement of Blood Pressure. Critically ill patients who require continuous monitoring of the blood pressure may have a catheter inserted into an artery and attached to a catheter-monitor-transducer system. The blood pressure is displayed on an oscilloscope at the bedside so that the patient's pressure can be determined at a glance. This intra-arterial technique of blood pressure monitoring provides accurate, objective, and continuous data on the patient's status.
blood pressure, mean arterial MAP; the average pressure within an artery over a complete cycle of one heartbeat; in the brachial artery, calculated to be the diastolic pressure plus 1/3 of the difference between the systolic and diastolic pressures.
blood stream bloodstream.
blood urea nitrogen see urea nitrogen.
blood volume
1. the total quantity of blood in the body; the plasma volume added to the red cell volume.
2. a laboratory test performed to determine this. The indicators used to determine these measurements are 125I-labeled human serum albumin for plasma volume and 51Cr-labeled erythrocytes for red cell volume. The regulation of blood volume in the circulatory system is affected by the intrinsic mechanism for fluid exchange at the capillary membranes and by hormonal influences and nervous reflexes that affect the excretion of fluids by the kidneys. A rapid decrease in the blood volume, as in hemorrhage, greatly reduces the cardiac output and creates a condition called shock or circulatory shock. Conversely, an increase in blood volume, as when there is retention of water and salt in the body because of renal failure, results in an increase in cardiac output. The eventual outcome of this situation is increased arterial blood pressure.
The blood volume in the pulmonary circulation is approximately 12 per cent of the total blood volume. Such conditions as left-sided heart failure and mitral stenosis can greatly increase the pulmonary blood volume while decreasing the systemic volume. As would be expected, right-sided heart failure has the opposite effect. The latter condition has less serious effects because the volume of the systemic circulation is about seven times that of the pulmonary circulation and it is therefore better able to accommodate a change in fluid volume.
The blood volume in the pulmonary circulation is approximately 12 per cent of the total blood volume. Such conditions as left-sided heart failure and mitral stenosis can greatly increase the pulmonary blood volume while decreasing the systemic volume. As would be expected, right-sided heart failure has the opposite effect. The latter condition has less serious effects because the volume of the systemic circulation is about seven times that of the pulmonary circulation and it is therefore better able to accommodate a change in fluid volume.
Tests. Clinical assessment of blood volume can be accomplished in a number of ways, for example, by measuring the patient's blood pressure while he is lying down, sitting, and standing. The quality and volume of peripheral pulses will give information about blood volume, as does determining the ease and speed with which a compressed vein will refill after pressure is released. Neck veins that are engorged indicate hypervolemia; the collapse of these veins indicates hypovolemia. A more accurate assessment can be done through the use of intravascular catheters such as the central venous pressure catheter, which measures pressure in the right atrium, and the swan-ganz catheter, which measures pressure on both sides of the heart.
Measurement of blood volume is accomplished by using substances that combine with red blood cells, for example, iron, chromium, and phosphate, or substances that combine with plasma proteins. In either case the measurement of the blood volume is based on the “dilution” principle. That is, the volume of any fluid compartment can be measured if a given amount of a substance is dispersed evenly in the fluid within the compartment, and then the extent of dilution of the substance is measured.
For example, a small amount of radioactive chromium (51Cr), which is widely used to determine blood volume, is mixed with a sample of blood drawn from the patient. After about 30 minutes the 51Cr will have entered the red blood cells. The sample with the tagged red blood cells is then returned by injection into the patient's bloodstream. About 10 minutes later a sample is removed from the patient's circulating blood and the radioactivity level of this sample is measured. The total blood volume is calculated according to this formula:
When volume is used to arrive at the total blood volume, a dye (usually T-1824, also known as Evans blue) is injected into the circulating blood. The dye immediately combines with the blood proteins and within 10 minutes is dispersed throughout the circulatory system. A sample of blood is then drawn and the exact quantity of dye is measured. Using the information about plasma volume obtained by applying the above formula, the total blood volume can be calculated, provided the hematocrit is also known. The formula for this calculation is:Measurement of blood volume is accomplished by using substances that combine with red blood cells, for example, iron, chromium, and phosphate, or substances that combine with plasma proteins. In either case the measurement of the blood volume is based on the “dilution” principle. That is, the volume of any fluid compartment can be measured if a given amount of a substance is dispersed evenly in the fluid within the compartment, and then the extent of dilution of the substance is measured.
For example, a small amount of radioactive chromium (51Cr), which is widely used to determine blood volume, is mixed with a sample of blood drawn from the patient. After about 30 minutes the 51Cr will have entered the red blood cells. The sample with the tagged red blood cells is then returned by injection into the patient's bloodstream. About 10 minutes later a sample is removed from the patient's circulating blood and the radioactivity level of this sample is measured. The total blood volume is calculated according to this formula:
whole blood that from which none of the elements has been removed, sometimes specifically that drawn from a selected donor under aseptic conditions, containing citrate ion or heparin, and used as a blood replenisher.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
Word not found in the Dictionary and Encyclopedia.
Latest Searches:
zygomaticofrontal - zygomaticofacialis - zygomaticofacial - zygomaticoauricular - zygomatico - zygomatici - zygomatica - zygomatic - zygoma - zygomas - zygodactyly - Zygocotyle - zygion - zygia - zygapophysis - zygapophysiales - zygapophysial - zygapophyseales - zygapophyseal - zygal -
- Service manuals - MBI Corp