Medical term:
hydroperitoneum
ascites
[ah-si´tēz]abnormal accumulation of serous fluid (edema) within the peritoneal cavity. It may be associated with any of numerous disorders, including neoplastic and inflammatory disorders of the peritoneum that produce increased permeability of the peritoneal capillaries; severe hypoalbuminemia from any cause; portal hypertension associated with cirrhosis of the liver, advanced congestive heart failure, and constrictive pericarditis; and hyperaldosteronism with increased retention of sodium and water. adj., adj ascit´ic.
In portal hypertension there is increased pressure within the sinusoids and hepatic veins. As the pressure increases there is movement of protein-rich plasma filtrate into the hepatic lymphatics. Some of the fluid enters the thoracic duct, but if the pressure is high enough, the excess fluid will ooze from the surface of the liver into the peritoneal cavity. Because the fluid has a high colloidal osmotic pressure owing to its high protein content, it is not readily reabsorbed from the peritoneal cavity.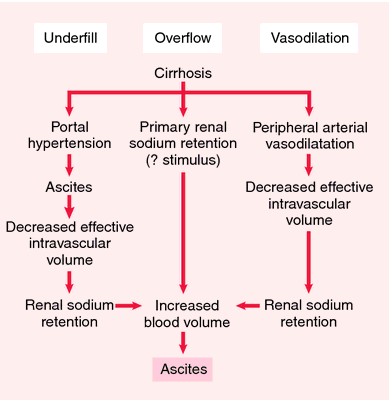
 (see accompanying illustration), recording daily weight gain and loss, and determining the extent to which pressure from the fluid is interfering with respiration, circulation, and digestion. Most patients with ascites are more comfortable in high Fowler's position. When a change of position is necessary to maintain integrity of the skin and promote circulation, small pillows can be used to support the rib cage while the patient is lying on the side. Ascites is usually a chronic condition that is difficult to control. Management must include instruction to the patient and significant others, particularly the caregivers who will help with home care.
(see accompanying illustration), recording daily weight gain and loss, and determining the extent to which pressure from the fluid is interfering with respiration, circulation, and digestion. Most patients with ascites are more comfortable in high Fowler's position. When a change of position is necessary to maintain integrity of the skin and promote circulation, small pillows can be used to support the rib cage while the patient is lying on the side. Ascites is usually a chronic condition that is difficult to control. Management must include instruction to the patient and significant others, particularly the caregivers who will help with home care.
In portal hypertension there is increased pressure within the sinusoids and hepatic veins. As the pressure increases there is movement of protein-rich plasma filtrate into the hepatic lymphatics. Some of the fluid enters the thoracic duct, but if the pressure is high enough, the excess fluid will ooze from the surface of the liver into the peritoneal cavity. Because the fluid has a high colloidal osmotic pressure owing to its high protein content, it is not readily reabsorbed from the peritoneal cavity.
Treatment. Because ascites is symptomatic of an underlying disorder that can range from liver failure to endocrine disease, treatment of the primary disorder is a major goal. The problems of fluid and electrolyte imbalance that are associated with ascites, and the potential for mechanical trauma due to pressure against internal organs adjacent to the abdominal cavity necessitate some kind of symptomatic relief.
Medical treatment includes restriction of fluid and sodium intake and administration of diuretics. Supplementation of potassium and chloride may be necessary during diuretic therapy to avoid an imbalance of these electrolytes. Careful measurement of intake and output is essential, and laboratory values for the electrolytes must be monitored frequently.
Surgical treatment was at one time almost entirely limited to abdominal paracentesis for removal of large accumulations of ascitic fluid. It is, however, only a temporary measure that poses problems of rapid fluid shift, loss of protein, and the potential for introducing infectious agents into the peritoneum. A more effective procedure is the insertion of a peritoneovenous shunt (LeVeen shunt), which provides a means for continuous reinfusion of ascitic fluid into the venous system.
Medical treatment includes restriction of fluid and sodium intake and administration of diuretics. Supplementation of potassium and chloride may be necessary during diuretic therapy to avoid an imbalance of these electrolytes. Careful measurement of intake and output is essential, and laboratory values for the electrolytes must be monitored frequently.
Surgical treatment was at one time almost entirely limited to abdominal paracentesis for removal of large accumulations of ascitic fluid. It is, however, only a temporary measure that poses problems of rapid fluid shift, loss of protein, and the potential for introducing infectious agents into the peritoneum. A more effective procedure is the insertion of a peritoneovenous shunt (LeVeen shunt), which provides a means for continuous reinfusion of ascitic fluid into the venous system.
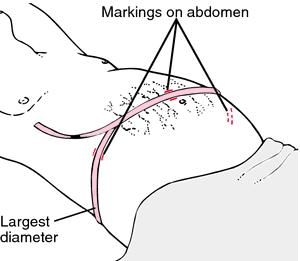
Patient Care. Assessment of the degree of fluid accumulation and the problems it presents to the patient can be done by measuring abdominal girth

Pathogenesis of ascites: different theories. Three important factors in the production of ascites in cirrhosis are portal hypertension, hypoalbuminemia, and hepatic blockage of lymphatic flow with local overproduction. From Aspinall and Taylor-Robinson, 2001.

How to measure abdominal girth of a patient with ascites. With patient supine, the tape measure is brought around the largest diameter of the abdomen and a measurement is taken. Before the tape is removed, the abdomen is marked along the sides of the tape on the flanks (sides) and midline to ensure that later measurements are taken in a consistent manner. Redrawn from Ignatavicius and Workman, 2002.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
as·ci·tes
(ă-sī'tēz),Accumulation of serous fluid in the peritoneal cavity.
Synonym(s): abdominal dropsy, hydroperitoneum, hydroperitonia
[L. fr. G. askos, a bag, + -ites]
Farlex Partner Medical Dictionary © Farlex 2012
as·ci·tes
(ă-sī'tēz)Accumulation of serous fluid in the peritoneal cavity. May be a complication of cirrhosis, congestive heart failure, malignancy, or peritonitis.
Synonym(s): hydroperitoneum, hydroperitonia.
Synonym(s): hydroperitoneum, hydroperitonia.
[L. fr. G. askos, a bag, + -ites]
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
hydroperitoneum
Excess fluid in the PERITONEAL CAVITY.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005
Patient discussion about hydroperitoneum
Q. Does ascites mean it's the end? My mother, age 65 was diagnosed with ovarian cancer in a routine US examination. It was also diagnosed she already has mild ascites. Does that mean her cancer is metastatic?
A. Ascites can render the staging of the cancer as metastatic, but it depends on the specific characters of the ascites, so further testing is needed here.
More discussions about hydroperitoneumThis content is provided by iMedix and is subject to iMedix Terms. The Questions and Answers are not endorsed or recommended and are made available by patients, not doctors.
ascites
[ah-si´tēz]abnormal accumulation of serous fluid (edema) within the peritoneal cavity. It may be associated with any of numerous disorders, including neoplastic and inflammatory disorders of the peritoneum that produce increased permeability of the peritoneal capillaries; severe hypoalbuminemia from any cause; portal hypertension associated with cirrhosis of the liver, advanced congestive heart failure, and constrictive pericarditis; and hyperaldosteronism with increased retention of sodium and water. adj., adj ascit´ic.
In portal hypertension there is increased pressure within the sinusoids and hepatic veins. As the pressure increases there is movement of protein-rich plasma filtrate into the hepatic lymphatics. Some of the fluid enters the thoracic duct, but if the pressure is high enough, the excess fluid will ooze from the surface of the liver into the peritoneal cavity. Because the fluid has a high colloidal osmotic pressure owing to its high protein content, it is not readily reabsorbed from the peritoneal cavity. (see accompanying illustration), recording daily weight gain and loss, and determining the extent to which pressure from the fluid is interfering with respiration, circulation, and digestion. Most patients with ascites are more comfortable in high Fowler's position. When a change of position is necessary to maintain integrity of the skin and promote circulation, small pillows can be used to support the rib cage while the patient is lying on the side. Ascites is usually a chronic condition that is difficult to control. Management must include instruction to the patient and significant others, particularly the caregivers who will help with home care.
In portal hypertension there is increased pressure within the sinusoids and hepatic veins. As the pressure increases there is movement of protein-rich plasma filtrate into the hepatic lymphatics. Some of the fluid enters the thoracic duct, but if the pressure is high enough, the excess fluid will ooze from the surface of the liver into the peritoneal cavity. Because the fluid has a high colloidal osmotic pressure owing to its high protein content, it is not readily reabsorbed from the peritoneal cavity.
Treatment. Because ascites is symptomatic of an underlying disorder that can range from liver failure to endocrine disease, treatment of the primary disorder is a major goal. The problems of fluid and electrolyte imbalance that are associated with ascites, and the potential for mechanical trauma due to pressure against internal organs adjacent to the abdominal cavity necessitate some kind of symptomatic relief.
Medical treatment includes restriction of fluid and sodium intake and administration of diuretics. Supplementation of potassium and chloride may be necessary during diuretic therapy to avoid an imbalance of these electrolytes. Careful measurement of intake and output is essential, and laboratory values for the electrolytes must be monitored frequently.
Surgical treatment was at one time almost entirely limited to abdominal paracentesis for removal of large accumulations of ascitic fluid. It is, however, only a temporary measure that poses problems of rapid fluid shift, loss of protein, and the potential for introducing infectious agents into the peritoneum. A more effective procedure is the insertion of a peritoneovenous shunt (LeVeen shunt), which provides a means for continuous reinfusion of ascitic fluid into the venous system.
Medical treatment includes restriction of fluid and sodium intake and administration of diuretics. Supplementation of potassium and chloride may be necessary during diuretic therapy to avoid an imbalance of these electrolytes. Careful measurement of intake and output is essential, and laboratory values for the electrolytes must be monitored frequently.
Surgical treatment was at one time almost entirely limited to abdominal paracentesis for removal of large accumulations of ascitic fluid. It is, however, only a temporary measure that poses problems of rapid fluid shift, loss of protein, and the potential for introducing infectious agents into the peritoneum. A more effective procedure is the insertion of a peritoneovenous shunt (LeVeen shunt), which provides a means for continuous reinfusion of ascitic fluid into the venous system.
Patient Care. Assessment of the degree of fluid accumulation and the problems it presents to the patient can be done by measuring abdominal girth
Pathogenesis of ascites: different theories. Three important factors in the production of ascites in cirrhosis are portal hypertension, hypoalbuminemia, and hepatic blockage of lymphatic flow with local overproduction. From Aspinall and Taylor-Robinson, 2001.
How to measure abdominal girth of a patient with ascites. With patient supine, the tape measure is brought around the largest diameter of the abdomen and a measurement is taken. Before the tape is removed, the abdomen is marked along the sides of the tape on the flanks (sides) and midline to ensure that later measurements are taken in a consistent manner. Redrawn from Ignatavicius and Workman, 2002.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
as·ci·tes
(ă-sī'tēz),Accumulation of serous fluid in the peritoneal cavity.
Synonym(s): abdominal dropsy, hydroperitoneum, hydroperitonia
[L. fr. G. askos, a bag, + -ites]
Farlex Partner Medical Dictionary © Farlex 2012
as·ci·tes
(ă-sī'tēz)Accumulation of serous fluid in the peritoneal cavity. May be a complication of cirrhosis, congestive heart failure, malignancy, or peritonitis.
Synonym(s): hydroperitoneum, hydroperitonia.
Synonym(s): hydroperitoneum, hydroperitonia.
[L. fr. G. askos, a bag, + -ites]
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
hydroperitoneum
Excess fluid in the PERITONEAL CAVITY.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005
Patient discussion about hydroperitoneum
Q. Does ascites mean it's the end? My mother, age 65 was diagnosed with ovarian cancer in a routine US examination. It was also diagnosed she already has mild ascites. Does that mean her cancer is metastatic?
A. Ascites can render the staging of the cancer as metastatic, but it depends on the specific characters of the ascites, so further testing is needed here.
More discussions about hydroperitoneumThis content is provided by iMedix and is subject to iMedix Terms. The Questions and Answers are not endorsed or recommended and are made available by patients, not doctors.
Latest Searches:
zygomaticofrontal - zygomaticofacialis - zygomaticofacial - zygomaticoauricular - zygomatico - zygomatici - zygomatica - zygomatic - zygoma - zygomas - zygodactyly - Zygocotyle - zygion - zygia - zygapophysis - zygapophysiales - zygapophysial - zygapophyseales - zygapophyseal - zygal -
- Service manuals - MBI Corp